
Case Report | DOI: https://doi.org/10.31579/2578-8868/152
1* Clinical Research Department, Centro Medico Nacional “20 de Noviembre”, ISSSTE, Mexico City
2 President of AMCEMIG (Asociación Mexicana para el Estudio de la Cefalea y Migraña), Mexico City
3 Neurology Department, Medicine Faculty, Universidad Autonoma de San Luis Potosi, México
*Corresponding Author: Rodriguez-Leyva Ildefonso, Neurology Department, Medicine Faculty, Universidad Autonoma de San Luis Potosi, México
Citation: García Silvia, Velez-Jimenez Karina, Rodriguez-Leyva Ildefonso. (2021) Migrainous Vertigo. An Approach. J. Neuroscience and Neurological Surgery. 8(1); DOI:10.31579/2578-8868/152
Copyright: © 2021 Rodriguez-Leyva Ildefonso, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 23 December 2020 | Accepted: 29 December 2020 | Published: 08 January 2021
Keywords: migraine; vertigo; migrainous vertigo; comorbility; dizziness
Background: Migraine and vertigo are highly prevalent; their simultaneous presentation is frequent and may require a different diagnostic approach than that used for migraine and vertigo separately. Migraine vertigo is recognized as a defined entity within the IHS classification of headaches.
Methods: We reviewed the principal manifestations of peripheral and central affection (brainstem) that explain this clinical picture presentation, reviewed the general characteristics, epidemiology, semiology, treatment and prognosis.
Results: The symptomatology suggest that the pathophysiology occurs as a vascular problem with aseptic inflammation and also affects the posterior territory. Although the condition's evolution is usually favorable, its dramatic presentation requires a detailed diagnostic approach (clinical and image), although the treatment does not differ from migraine's general management.
Conclusion: The vestibular migraine or Migrainous Vertigo is an already defined entity, although the treatment is similar to the migraine with and without aura.
Both migraine and vertigo are common and both individually have a high prevalence in the general population; 16% for migraine and 7% for vertigo. [1] The expected concurrency would be 4 % of the general population by pure chance.(2) The epidemiological evidence suggests that one of each four subjects with benign paroxysmal positional vertigo (BPPV) have migraine. [3] The differential diagnosis includes benign paroxysmal positional vertigo, Meniere's disease, cerebellar disorders, and anxiety syndromes that may present with dizziness. [4]
Migrainous vertigo (MV): vertigo directly caused by the migraine phenomenon, which can be said to affect more than 1% of the general population. [5]
MV presents with attacks of spontaneous or positional vertigo lasting from seconds to days. The pictures associate headache, phonophobia, photophobia, and auras with cochlear symptoms, which can be mild to moderate and even manifest with spontaneous or positional central nystagmus and frequently with unilateral vestibular hypofunction. [6]
In symptom-free intervals, the vestibular test has low diagnostic value since the findings are non-specific. MV treatment is adopted in migraine, which includes avoidance of triggers, stress management, and pharmacotherapy for acute attacks, and of course, prophylaxis to avoid relapses. [7]
EPIDEMIOLOGY
The MV is the most common cause of vertigo in adults. It has a prevalence of 1 to 2.7%. [8] It predominates in women (2-6 / 1). It mainly affects the population between the third and fourth decade of life. The patient usually has a family history of migraines, and the sufferer usually has motion sickness (the patient quickly becomes motion sick). [9]
DIAGNOSTIC APPROACH
The diagnosis of vestibular migraine is predominantly clinical, based on family history and the recurrent presence of vestibular and migraine symptoms. [10]
The temporal association between vestibular symptoms and migraine manifestations are intermittent and with the adequate exclusion of other causes of vestibular problems. Symptoms required for the diagnosis of vestibular migraine include various types of vertigo and dizziness induced by movements of the head, with associated nausea. [11]
Symptoms are usually moderate or severe in intensity. The duration of the episodes is limited to a period between 5 minutes and 72 hours, according with the IHS Diagnostic Criteria. [12] They are covered in section A1.6.6 Vestibular migraine (The previously used terms were: vertigo associated with migraine/dizziness; vestibulopathy related to migraine; migraine vertigo). [11]
DIAGNOSTIC CRITERIA
A. At least five episodes meeting criteria with vestibular symptoms of moderate or severe intensity, lasting between five minutes and 72 hours and at least half of the episodes are associated with at least one of the following three migraine characteristics: 1. headache with at least two of the following characteristics: a) unilateral location, b) pulsating quality, c) moderate or severe intensity, d) aggravation from routine physical activity. Besides, photophobia and phonophobia. A visual aura can be present or not. But something indispensable is that it cannot be better explained by another ICHD-3 diagnosis or by another vestibular disorder. This diagnosis must especially be considered when a current or history of migraine without aura or Migraine with aura is present. [12]
Therefore, at least five episodes of vestibular symptoms of moderate to severe intensity, lasting between 5 minutes to 72 hours, with a current or previous history of migraine with or without aura according to the ICDH. One or more migraine features in at least 50% of vestibular episodes:
Headache with at least two of the following characteristics: unilateral, throbbing, pain of moderate or severe intensity, with aggravation to routine physical activity, photophobia and phonophobia and the presence of visual aura, can be present. [11]
It is important to note that the symptoms should not be attributed to another vestibular disease or to a diagnosis that falls under another section of the ICDH. [9]
There are a synonymies for this entity, among these are; a) Migraine vertigo, b) Vertiginous migraine c) Migraine associated with vertigo, d) Migraine associated with dizziness, e) Migraine associated with vestibulopathy, f) Benign recurrent vertigo [11]
The presentation before the provocation of an episode can be an essential clue for VM diagnosis; positional changes, visual stimuli, rapid movements of the head, menstruation, stress, lack of sleep, dehydration, and certain foods can trigger migraine attacks. The sensitivity and specificity of each of these precipitating factors have not been adequately studied. [13]
CLINICAL PICTURE
A good portion of patients has a family history of migraine. The main clinical manifestations are the presence of a throbbing headache, associated with photophobia, sonophobia (90%), nausea (80%), and very frequently anxiety (70%); more than half of those who suffer it present vertigo and a third part present a feeling of dizziness. Motion sickness is present in two out of every three migraineurs; the picture is like migraine, more frequent in women and even more during menstruation. [14]
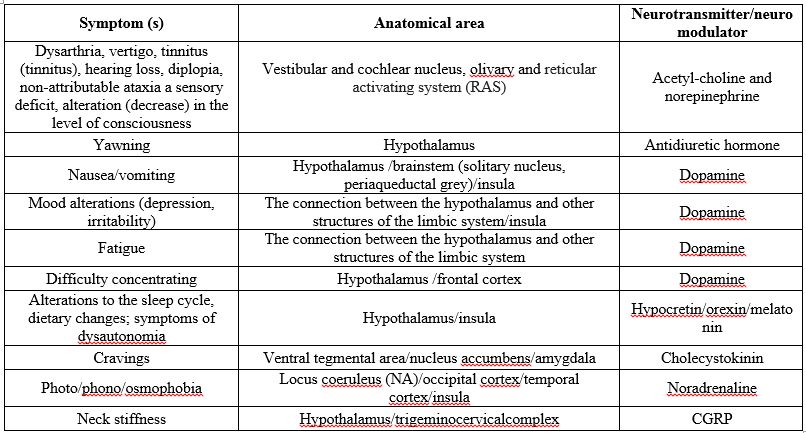
Aura can present as tinnitus, associated or not with muffling of sound, auditory pain, visual or sensitive aura. It can also present as a brain stem aura (1.1.2) ICHD-3, being considered typical if at least two manifestations of the brainstem present and revert (dysarthria, vertigo, tinnitus (tinnitus), hearing loss, diplopia, non-attributable ataxia a sensory deficit, alteration (decrease) in the level of consciousness (GCS score less than 13 points), without the presence of motor or retinal symptoms. It is important to always consider that the migraine aura lasts from 5 to 60 minutes and is usually accompanied by a headache. [15]
The vestibular manifestations are vertigo, dizziness, rocking, inclination, falling sensation, floating sensation, wiggling, sliding, multidirectional movement, positional vertigo. [11]
The characteristics of headache in MV are that it occurs between 1 to 3 out of 4 of the cases (therefore, its absence does not rule out vestibular migraine). It is usually less severe than in common migraine, and vertigo is frequently more prominent, visual aura occurs in one-third of patients. Photophobia and sonophobia are found in 70 to 90% of cases. [8] Figure 1.
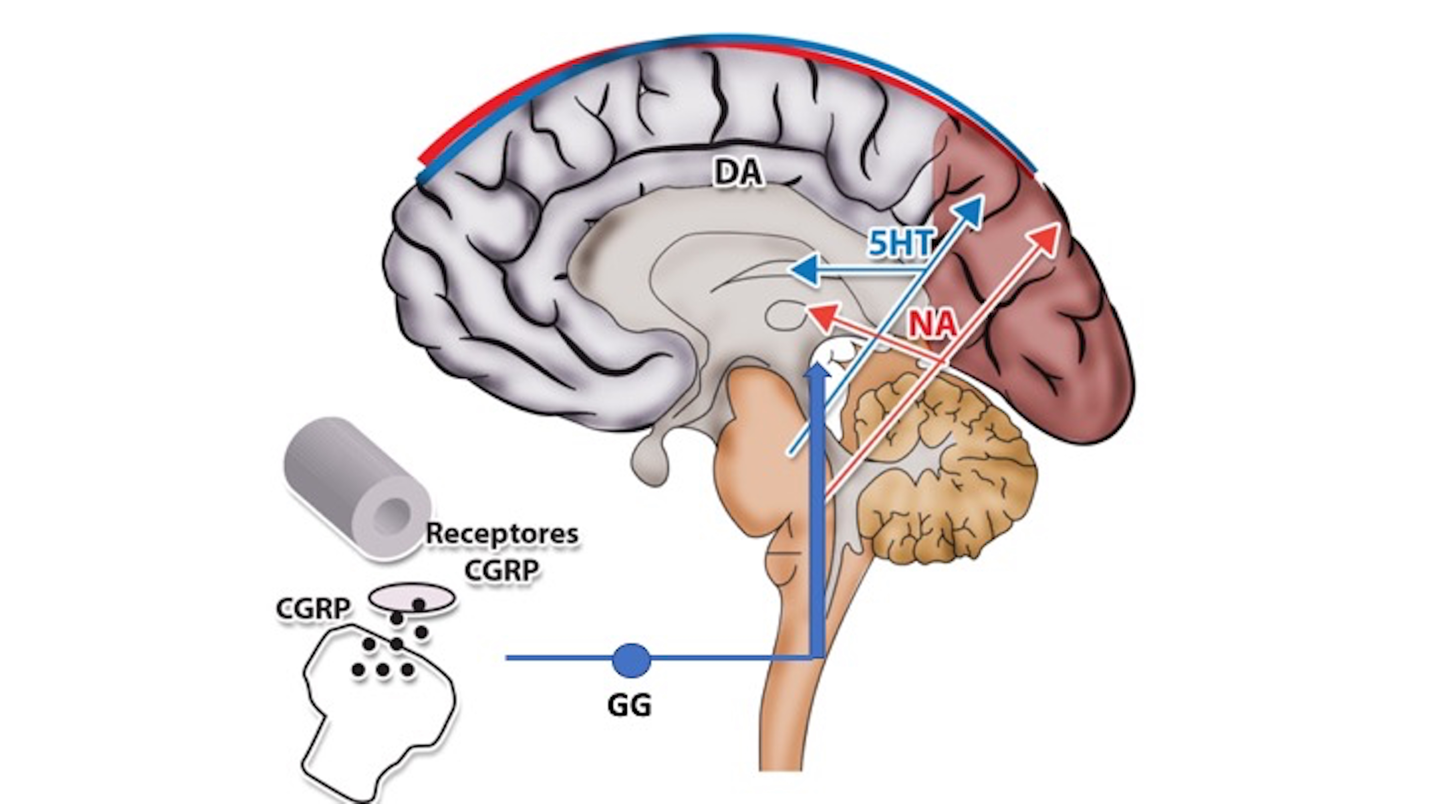
Migraine etiology is unknown, and its pathophysiology remains unclear; however, the trigeminal-vascular complex (TCC) seems to be the cornerstone of physiological alterations in vestibular migraine. Migraine must be approached as a complex disorder of brain networks on to genetic basis; its symptoms involve the multiple cortical, subcortical, and especially brainstem regions. [16]
Migraine is a neuronal networks disorder in subcortical and cortical brain circuits involved in headache and a deficient sensory processing; it is controversial if these changes are genetically determined or due to chronic pain and vestibular manifestations; in fact, all are possible. Three genetic markers are consistent in association with MV: rs2651899 in the PRDM16 gene, rs10166942 in theTRPM8 gene, and rs11172113 in the LRP1 gene. Several structures in the peripheral and central nervous system are involved; meninges, trigeminal nerve, vascular anterior and posterior (vertebrobasilar) system, trigemino-cervical complex, multiple nucleus of the brainstem, hypothalamus, thalamus and cerebral cortex. [17]
According to the current scientific migraine perspective, this analysis was divided into a) inter-ictal stage (brain alterations in migraine people, without migraine and vestibular attack); b) ictal stage. [18]
DIFFERENTIAL DIAGNOSIS
The differential diagnoses that we must include are 1. Meniere's disease, 2. Somatoform vertigo (primary or secondary that develops after vestibular vertigo) 3. Benign paroxysmal positional vertigo (BPPV) 4. Transient cerebral ischemia of the posterior circulation (TIA), 5.Syncope and orthostatic hypotension, 6. Vestibular paroxysm, and 7. Type 2 episodic ataxia.(20)
Benign paroxysmal positional vertigo and vestibular migraine can present only with positional vertigo, thus mimicking benign paroxysmal positional vertigo (BPPV).
Differentiation may require direct clinical observation of nystagmus during the acute phase. In vestibular migraine, the positional nystagmus is usually persistent and does not align with an isolated semicircular canal. Symptomatic episodes tend to be shorter in vestibular migraine (minutes to days rather than weeks) and more frequent (several times a year in vestibular migraine instead of once every several years in BPPV). [21]
Vertebrobasilar transient ischemic attacks (TIA) should be considered in the differential diagnosis, especially in older patients, if there are vascular risk factors, sudden onset of symptoms, less than one year of full attack history, and evidence of vascular disease in the vertebral or basilar arteries demonstrated by CT angiography, MRI angiography or Doppler ultrasound. [22]
Vestibular Paroxysmia is a controversial disorder caused by vascular compression of the vestibular nerve. It presents as brief vertigo attacks, lasting between one and several seconds, recurring several times a day, and associated with hemifacial spasm. Successful prevention of seizures using carbamazepine or oxcarbazepine supports the diagnosis. [23]
Psychiatric dizziness is associated with anxiety and depression and can cause dizziness and complicate a vestibular disorder's diagnosis. Anxiety-related dizziness is characterized by its occurrence in specific situations, hyperventilation, autonomic activation, catastrophic thinking, and avoidance behavior. [9]
Meniere's Disease usually presents with vertigo episodes, associated with tinnitus and hearing loss. As this picture repeats itself the hearing loss increases, initially unilaterally but with time, both ears are affected. Differential diagnosis is complicated because half of the patients with Meniere have a migraine, and besides, half of the patients with a Meniere attack will then have a migraine. Meniere's disease is distinguished from vestibular migraine because sensorineural deafness is seldom unilateral. Discrete bilateral deafness can be found more in MV. It also affects more women with less difference than MV vertigo, usually between 20 minutes and 12 hours. However, the differential diagnosis can be difficult. [24]
INTERICTAL MANIFESTATIONS (VESTIBULAR)
Dizziness can often be induced visually in 9 out of 10 patients; it can also present with head movement in 6 out of 10 patients, benign positional vertigo reproduces in 1 out of 10 patients, and paroxysmal vestibular symptoms occur in 10% of patients. In contrast, dizziness can become persistent in half of all patients. [25]
TREATMENT
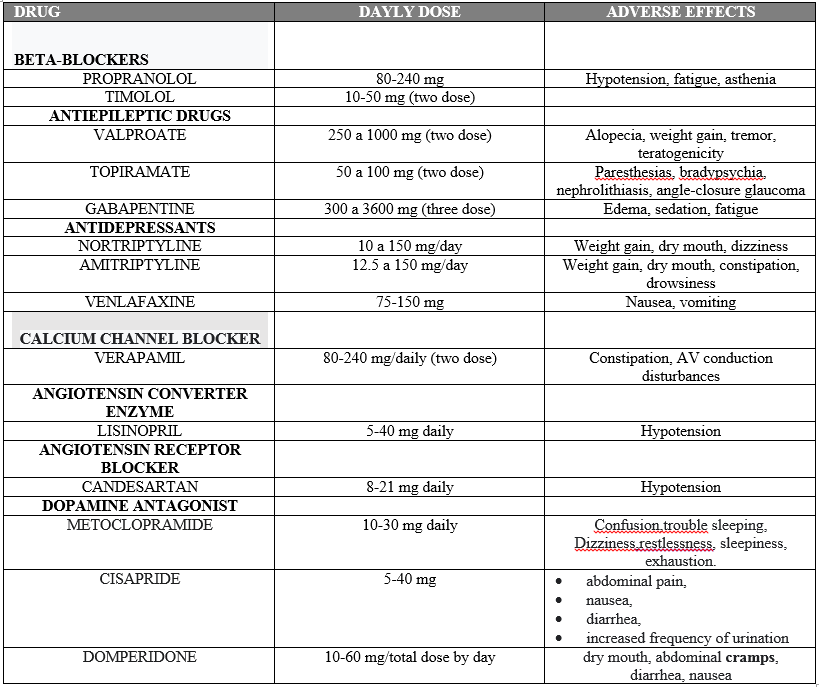
The dietary hygiene measures mainly include avoiding wakefulness, foods with aspartame, monosodium glutamate, and tyramine, perfume odors, head trauma, and sudden changes in position— climbing heights or rides. [26] Once the acute attack has occurred, we can administer the traditional treatment, which we could divide into a) Non-specific (NSAIDs) and b) specific (triptans) and add the new therapeutic options that we now have: 1. Gepantes (ubrogepant, rimegepant) and 2. Lasmidatan. When the symptoms occur with a frequency greater than three per month, it may be necessary to propose to the patient to use preventive management: a) Traditional: antidepressants (tricyclics, IRSS), beta-blockers (propranolol), Ca channel blockers (verapamil, flunarizine) and the new drugs, molecularly explicitly designed for the treatment of migraine: monoclonal antibodies directed at the CGRP receptor or ligand. [27]
Of course, the management of comorbidities is mandatory. Sometimes we can choose a prophylactic that helps us control both problems, for example, for depression, an IRSS, for anxiety if a tricyclic such as imipramine is not very important, for overweight, we can use an antiepileptic such as topiramate; for hypertension, a beta-blocker such as propranolol or a Calcium channel blocker such as verapamil. It may be necessary to associate an antiemetic (metoclopramide) in these patients, if anxiety is significant a benzodiazepine, and sometimes if the manifestations are very severe antidopaminergic (chlorpromazine). [26]
CHRONIC VESTIBULAR MIGRAINE
Vestibular migraine is broadly conceptualized as episodic. However, a chronic variant has been described; although this situation seems to be more theoretical, many neurologists have faced it. The distinction between chronic vestibular migraine and comorbidity syndromes such as psychiatric dizziness can be challenging. In the future, chronic vestibular migraine may become a formally recognized category within the ICHD. [29]
Vestibular migraine is a common problem. Although there are well-defined diagnostic criteria, concluding the problem is not easy. The manifestations of vestibular dysfunction are characteristic and multiple. Treatment does not differ from the management of migraines. This diagnosis is undoubtedly an opportunity for medicine to define a better diagnostic and therapeutic approach to this fascinating and challenging problem.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
